What is Patella Femoral Pain Syndrome?
Patellofemoral pain syndrome (PFPS), often called “runner’s knee” or anterior knee pain, is a common condition. The differential diagnosis of PSFS includes chondromalacia and patellar tendonopathy. Chondromalacia patella is not classified within the broader category of PFPS, as its underlying pathophysiology differs and requires a distinct treatment approach.[1]
While chondromalacia patella may occur in individuals experiencing patellofemoral pain, not all cases of patellofemoral pain syndrome involve chondromalacia patella.[2]
It is often called 'Runner's Knee'
Anatomy of the Patella
The patella is the largest sesamoid bone in the body, embedded within the tendon of the quadriceps muscle group. It sits in the trochlear groove of the femur and acts as a pulley system for the knee. Superiorly, it is attached to the quadriceps tendon, which connects the four quadriceps muscles to the patella. Inferiorly, it continues as the patellar tendon (or ligament), attaching to the tibial tuberosity.
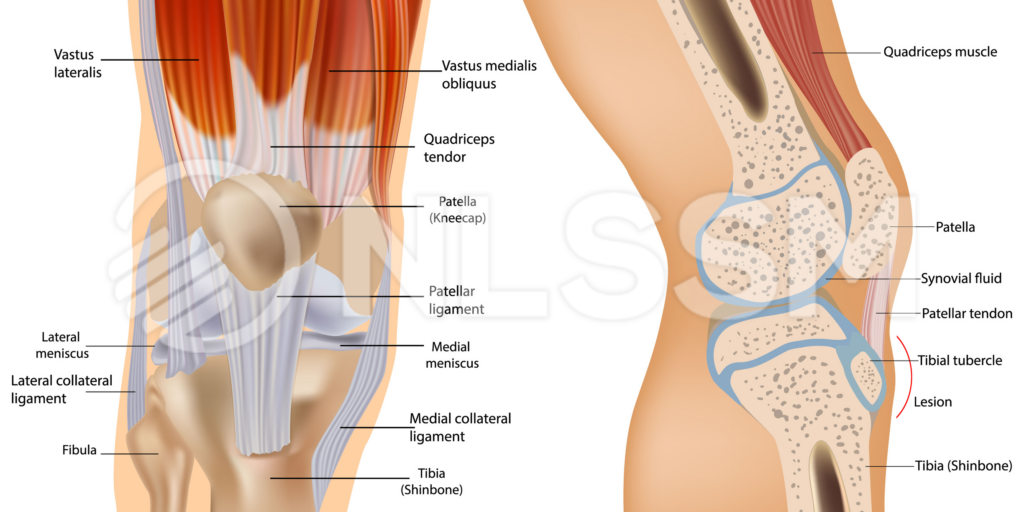
Medially and laterally, the patella is stabilised by the medial and lateral retinacula, as well as contributions from the vastus medialis oblique (VMO) and vastus lateralis. These soft tissue structures guide patellar tracking during knee flexion and extension.
Functionally, the patella increases the mechanical advantage of the quadriceps by improving the angle of pull, enhancing knee extension strength and efficiency. It also helps distribute compressive forces across the patellofemoral joint during activities such as squatting, running, and stair climbing.
Top 3 Potential Risk Factors for Patellofemoral Pain Syndrome (PFPS)
65% of PFPS is due to tracking or instability problems [Larson, Grana, 1993], but that being said, the mechanism is not fully understood. There are some thoughts on contributing factors:
1. Quadriceps weakness: poor quad strength alters patellar tracking and increases the risk of knee pain. [3]

2. Altered biomechanics / dynamic valgus: inward knee collapse during movement stresses the patellofemoral joint. [4]

3. Overuse & training errors – high running/jumping volume or sudden workload increases overload the joint. [5]

It’s also important to consider how movement patterns influence both patellofemoral pain (PFPS) and the potential development of a tendinopathy. The way an individual loads the knee during functional tasks can determine which structures are placed under greater stress. For example, pain that is worse on ascending stairs may indicate increased lateral patellar maltracking, often associated with tightness or overactivity in the ITB/TFL complex and/or inhibition or delayed activation of VMO.
Conversely, pain that is more pronounced when descending stairs is frequently linked to reduced quadriceps strength and poor eccentric control, leading to increased patellofemoral joint stress. Understanding these task-specific aggravating factors can help guide assessment and more targeted rehabilitation strategies.
How to assess it: Which assessment?
This is about building up your picture, layering your assessments with a combination of palpation, range of motion and functional tests.

Palpation: start with the medial and lateral borders of the patella to reveal any tenderness and rule out possible swelling. But you are also going to look more global, follow the lines of movement such as lateral structures, such as the vastus lateralis, lateral retinaculum, ITB and tensor fasciae latae / gluteal medius
PROM: the patella should be palpated for any crepitus and to check that the patella tracks in the same way, laterally, as it does in the active range.
Functional tests / AROM: Double Leg Squat is a great active range of motion test! Sensitivity 91% vs Specificity 51% [6]
What Your Hands Are Telling You
When palpation and movement point to PFPS, think beyond “tight muscles”.
- Lateral quad or TFL tenderness? Often reflects poor force control at the hip → increased stress at the patella.
- Reduce patellar sensitivity? More likely tissue irritability from load overload than structural damage.
- Pain on squats? Suggests reduced quadriceps load tolerance and altered knee mechanics.
Clinical Takeaway for Soft Tissue Therapists
Your treatment helps calm tone, improve movement tolerance, and restore confidence. And remember, long-term change comes from incorporating + supporting better loading and movement.
About The Author
This blog was written by NLSSM Manager, Cassandra Gramozi.
Since qualifying with NLSSM, Cassandra has worked with people from all walks of life including the Saracens RFC, private clinics and volunteered at the London 2012 Olympics.
After three seasons with the London Wasps RFC as their Senior Soft Tissue Therapist, she moved into the world of Olympic Sports and spent the next four years working in the United Kingdom Sports Institution (formerly EIS) and the Intensive Rehabilitation Unit dedicated to BOA-funded athletes.
She currently works for the Football Association as a consultant Soft Tissue Therapist to the U21’s Mens England Football team.
She is also a fully qualified Polestar Pilates Reformer instructor, and when she is not in the pilates studio, you can find her at NLSSM helping run the business on a day-to-day basis.

References
Click for References
- Wiles P, Andrews PS, Devas MB. Chondromalacia of the patella. Bone & Joint Journal. 1956 Feb 1;38(1):95-113.
- Willy RW, Hoglund LT, Barton CJ, Bolgla LA, Scalzitti DA, Logerstedt DS, Lynch AD, Snyder-Mackler L, McDonough CM. Patellofemoral Pain. J Orthop Sports Phys Ther. 2019 Sep;49(9):CPG1-CPG95. doi: 10.2519/jospt.2019.0302.
- Lankhorst NE, Bierma-Zeinstra SM, van Middelkoop M. Risk factors for patellofemoral pain syndrome: a systematic review. J Orthop Sports Phys Ther. 2012 Feb;42(2):81-94. doi: 10.2519/jospt.2012.3803. Epub 2011 Oct 25. PMID: 22031622.
- Petersen W, Rembitzki I, Liebau C. Patellofemoral pain in athletes. Open Access J Sports Med. 2017 Jun 12;8:143-154. doi: 10.2147/OAJSM.S133406. PMID: 28652829; PMCID: PMC5476763.
- Gaitonde DY, Ericksen A, Robbins RC. Patellofemoral Pain Syndrome. Am Fam Physician. 2019 Jan 15;99(2):88-94. PMID: 30633480.
- Double leg squat ref – Mostafaee, N. et al. (2024) ‘Examining the diagnostic accuracy of common physical examination and functional tests in the diagnosis of patellofemoral pain syndrome among patients with anterior knee pain’, Physiotherapy Theory and Practice, 40(4), pp. 843–855. doi: 10.1080/09593985.2022.2158053.