Written by Cassandra Gramozi, L5 SRMT
How structured assessment thinking helped guide rehabilitation after Achilles reconstruction
Most conversations about lower limb injuries in sport follow a familiar script where we talk about overload, tendinopathies, training errors, and cumulative stress injury as something that quietly creeps in over time.
This case didn’t follow that pattern at all. It was a full rupture, followed by a particularly unique surgery – a reinforced, accelerated repair technique [1] – that had only been performed in the UK a handful of times at this point.
It’s important to note that I didn’t meet the athlete at the beginning of their rehabilitation journey, I met them later in that sometimes uncomfortable, frustrating in-between stage. The stage where the surgery is technically successful, strength numbers are improving, but movement still doesn’t feel trustworthy. Where the body looks repaired on paper, but doesn’t yet behave like it believes that repair.
What this case ultimately taught me was the difference between repair and reconstruction, and why effective rehabilitation depends on thinking in systems, not segments.
The athlete and the environment
The athlete was a winter sport competitor in their mid-30s – fast, elastic, and explosively powerful. A sprint-pattern dominant mover who loaded their Achilles like a spring.
They had sustained a complete Achilles rupture during a training session. They then underwent surgical re-attachment using a wire fixation technique designed to tolerate earlier loading and accelerate return-to-performance benchmarks. The procedure is well documented in orthopaedic literature, and on paper, the outcomes are compelling [1]. And the reason for this was that the Winter Olympics were less than a year out and so time was not on our side.
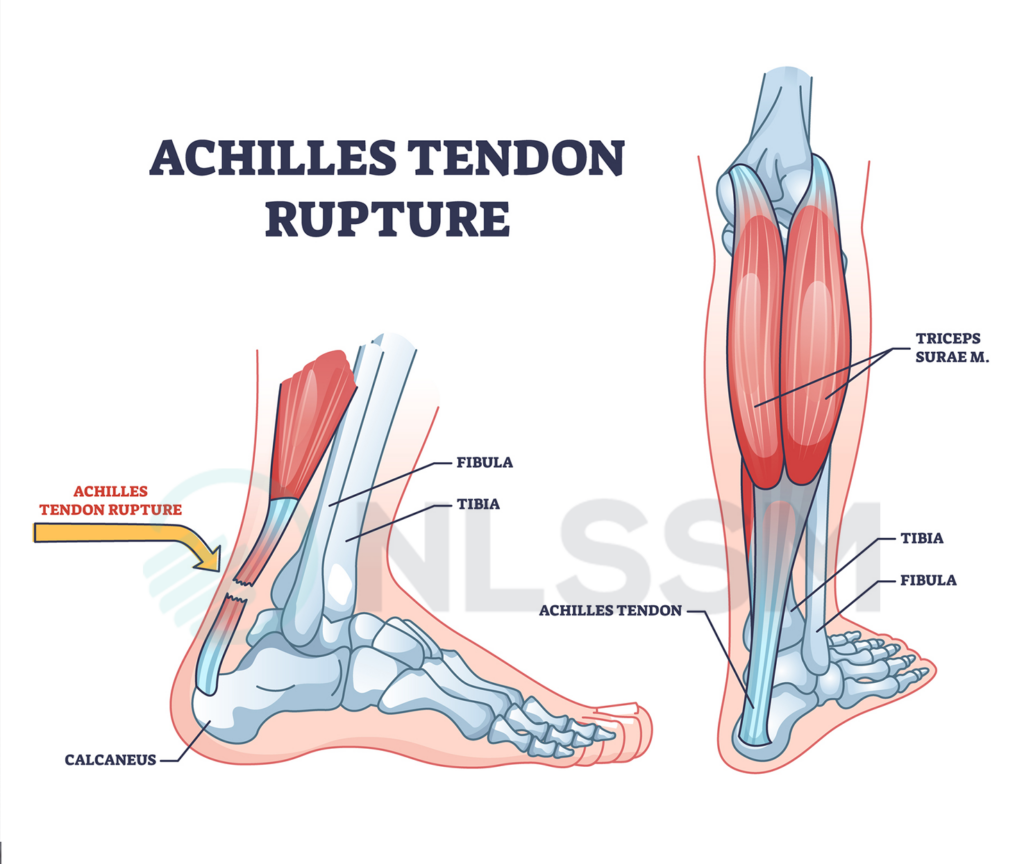
But here’s the reality that often gets lost: Repairing a tendon is one thing, re-teaching an entire lower limb to trust that tendon again is something else entirely!
I met them during the sub-acute phase of rehabilitation at the UK Sport Institute (UKSI) Intensive Rehabilitation Unit (IRU), based at Bisham Abbey National Sports Centre. The IRU offers residential, high-intensity rehabilitation for elite athletes within the British Olympic system, bringing together a full multidisciplinary team (MDT) under one roof.
With only a small number of athletes in residence at any one time, the model allows for deeply individualised care. For this athlete, that meant I was able to work with them twice a week over several months, an invaluable window into how change actually unfolded over time.
My role within the multidisciplinary team
Within the IRU, the athlete was supported by a full MDT: sports doctor, psychologist, nutritionist, strength & conditioning coach, and physiotherapist.
My remit was Soft Tissue Therapy. Now, it’s easy to reduce that role to “hands-on work” or to assume soft tissue input sits on the periphery of performance rehabilitation. But the way I practise, and the way we teach at NLSSM, demands structured clinical reasoning at every stage.
Soft Tissue Therapy in a high-performance return-to-sport pathway is not cosmetic, but rather it is targeted, hypothesis-led, and assessment-driven.
This is where I believe massage and soft tissue therapists need to step into a clearer professional identity of contributors to the decision-making ecosystem, not just passive technicians.
Session Outline / Thought Process
The MDT handover was thorough and collaborative. We were aligned on goals and constraints, but what emerged in the first hands-on session shifted the direction of the work.
On initial palpation, the athlete’s right anterior knee and plantar fascia felt tethered, not acutely tender, not inflamed, but stuck. This wasn’t local tissue irritation; it was the kind of immobility that comes from prolonged protection and lack of movement.
The boot had created a holding pattern and their body was behaving like a suspended puppet, like segments waiting for permission to move.

Crucially, the first breakthrough didn’t come from working directly on the Achilles, but from working everywhere around it.
We ran a structured assessment chain that included:
- Tissue mobility mapping through the calf, hamstrings, lateral hip and adductors
- Fascial glide and spacing between the 1st–3rd metatarsals (particularly relevant given the prolonged boot)
- Functional knee-to-wall testing or also known formally as weight weight-bearing lunge test [2], as a marker of weighted dorsiflexion tolerance
The knee-to-wall test became our primary outcome measure and it gave us an honest indicator of their willingness (not just ability) to load the chain. It was easy to repeat, visible to the athlete, and could be shared consistently across physio and gym sessions.
That consistency mattered, for both practitioners and the athlete.
Following treatment focused on fascial release through the anterior & posterior knee, plantar fascia, and thoracolumbar line, their knee-to-wall measure improved significantly within the session. Importantly, this change did not occur when we went straight to the site of injury.
The system, not the tendon, was holding the brakes.
What we actually did
Intervention evolved session by session, guided by reassessment. Techniques included:
- Soft Tissue Therapy (STT) through the posterior chain
Instrument-assisted STT through anterior and posterior knee structures, including the popliteus - Fascial mobilisation between the 1st and 3rd metatarsals
- Deep and soft tissue work through the thoracolumbar fascia and region of the right quadratus lumborum
- Intercostal spacing combined with breath-guided thoracic work
We also treated the left hip, not because it was “injured”, but because crutching and guarded weight transfer had quietly written compensatory patterns into the system.
After each intervention block, we retested and the pattern was remarkably consistent. This is often the point in workshops where newer therapists raise an eyebrow, but it’s worth saying clearly: Sometimes the solution lives nowhere near the scar.
The psychology mattered as much as the hands-on work

One of the most significant aspects of this case was the role Soft Tissue Therapy played as a bridge, both physiologically and neurologically.
While the surgery reconstructed the tendon, rehabilitation required the athlete to rebuild trust in movement. That process is rarely linear.
Touch, when delivered with consent, intention, and clinical reasoning, has a powerful influence on the nervous system – manual therapy can potentially help modulate pain perception, reduce threat, improve body awareness, and enhance engagement when paired with clear communication. [3] [4] [5]
But beyond the data, there was something else happening in the treatment space….
The room became somewhere the athlete wasn’t being tested or measured. It was a controlled environment where discomfort could be explored gradually, where pacing was respected, and where they could recalibrate their perception of load without performance pressure.
Soft Tissue Therapy allowed for graded exposure, influencing tone where protective holding patterns had developed and supporting interoceptive awareness. They learned to distinguish surgical sensation from protective tension, and protective tension from genuine overload.
I do believe that well-reasoned touch signals safety to the nervous system. It creates a platform upon which more demanding strength, power, and plyometric work can eventually be built.
In this way, STT became more than symptom management, but part of neuromuscular re-education and a bridge between immobilisation and confident movement.
The psychology mattered as much as the hands-on work
This is not a story about an exceptional individual, but rather, it’s a story about process.
The temptation after surgery is always to zero in on the site of repair. But that site is only one chapter in a much larger story and in this case, the real limiter wasn’t the tendon, it was the system surrounding it.
Had I treated the calf simply because “Achilles = calf”, this outcome would not have occurred.
The change came from following a chain of reasoning:
scar → boot → immobilisation → fascial tethering → altered gait → altered thoracic tension → load inhibition → reduced dorsiflexion → increased threat perception
We worked with the system, not the symptom. It highlights an important message for our profession: effective rehabilitation is not about isolated tissue work. When applied thoughtfully, Soft Tissue Therapy can influence both mechanical and neurological readiness, creating a safe space for movement to be relearned and confidence restored.
That requires more than technical skill. It requires structured assessment frameworks, integrated with palpation and clinical reasoning, so that intervention and reassessment inform each other continuously.
When that feedback loop is in place, touch becomes a tool for recovery at every level; tissue, system, and psyche.
Frequently Asked Questions
1. Why can movement still feel difficult after Achilles surgery?
As explored in this case, a successful surgical repair does not always mean movement immediately feels normal or trustworthy. During rehabilitation, strength may improve while confidence in loading and movement remains limited. In this athlete’s case, rehabilitation focused on how the wider lower limb system behaved, not just the repaired tendon itself.
2. What assessments are used during Achilles rehabilitation?
Assessment in this case included tissue mobility mapping through the calf, hamstrings, hip and adductors, fascial glide through the foot, and the knee-to-wall (weight-bearing lunge) test to assess weighted dorsiflexion tolerance. Reassessment was used throughout to guide treatment decisions and monitor change over time.
3. Can treatment away from the injury site help lower limb recovery?
In this case, meaningful changes occurred when treatment addressed structures surrounding the injury rather than focusing solely on the Achilles tendon. Areas including the knee, plantar fascia, thoracolumbar region, and hip were assessed and treated as part of a wider systems-based approach to rehabilitation.
4. What role can Soft Tissue Therapy play during sports injury rehabilitation?
Within this rehabilitation setting, Soft Tissue Therapy formed part of a multidisciplinary team approach. Treatment was assessment-led and reassessment-driven, working alongside physiotherapy, strength and conditioning, psychology, nutrition, and sports medicine during the athlete’s recovery process.
5. Why is a whole-body approach important in lower limb rehabilitation?
This case highlighted how surgery, immobilisation, altered gait, and compensatory movement patterns can influence the wider system. Rather than focusing only on the site of repair, rehabilitation considered how surrounding tissues and movement behaviours may contribute to confidence and tolerance to load over time.
References
- Byrne PA, Hopper GP, Wilson WT, Mackay GM. Knotless Repair of Achilles Tendon Rupture in an Elite Athlete: Return to Competition in 18 Weeks. J Foot Ankle Surg. 2017 Jan-Feb;56(1):121-124. doi: 10.1053/j.jfas.2016.07.007. Epub 2016 Aug 21. PMID: 27555353.
- Bowden CJ, Hoch JM, Hoch MC. Reliability and minimal detectable change of the weight-bearing lunge test: A systematic review.Man Ther. 2015 Aug;20(4):524-32 (last accessed 12 November 2018).
- Moseley GL, Flor H. Targeting cortical representations in the treatment of chronic pain: a review. Neurorehabil Neural Repair. 2012 Jul-Aug;26(6):646-52. doi: 10.1177/1545968311433209. Epub 2012 Feb 13. PMID: 22331213.
- Moseley GL, Nicholas MK, Hodges PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin J Pain. 2004 Sep-Oct;20(5):324-30. doi: 10.1097/00002508-200409000-00007. PMID: 15322439.
- G. Lorimer Moseley, David S. Butler, Fifteen Years of Explaining Pain: The Past, Present, and Future,The Journal of Pain,Volume 16, Issue 9, 2015,Pages 807-813, ISSN 1526-5900,
About the Author

Cassandra Gramozi | L5 SRMT
Joining in 2004, Cassandra saw first-hand the positive effects of sports massage and decided to take the course herself, graduating in 2008.
Since qualifying with NLSSM, Cassandra has worked with people from all walks of life including the Saracens RFC, private clinics, and participants in several London Marathons and the London 2012 Olympics.
Read More
After three seasons with the London Wasps RFC as their Senior Soft Tissue Therapist, she moved into the world of Olympic Sports and spent the next 4 years working in the English Institute of Sport and the Intensive Rehabilitation Unit dedicated to BOA funded athletes.
She currently works for the Football Association as a consultant Soft Tissue Therapist to the U21’s Mens England Football team.
Cassandra is also a fully qualified Polestar Pilates Reformer instructor and when she is not in the pilates studio you can find her at NLSSM helping run the business on a day to day basis.